Communication between teams, patients and informal caregivers
Downloaded content date
Communication between teams, patients and informal caregivers

Some people with a learning disability struggle to communicate when using only expressive or receptive language; however, there are alternative methods of communication.
Makaton and Picture Exchange Communication System (PECS) which uses easy to read symbols via systems such as Widgit or objects of reference.
When communicating with someone with a learning disability, it is important to allow additional time for the individual to understand the information and avoid jargon. To support conversations, it may be beneficial to create easy-to-read documents to aid information sharing.
A speech and language therapist may have assessed some individuals with a learning disability, or may have been previously assessed; this assessment outcome will help understand the individual's communication style and needs.
Hospital passport/health passport
Hospital passports are designed to provide key, valuable information to the clinician or person delivering care to someone with a learning disability. This should be completed proactively and is a patient-held document; therefore, the patient or their family/carers should bring the hospital passport with them to each health appointment.
The hospital passport should include information regarding how the patient may communicate, for example, verbally, Makaton, and so on. It should also include details about their individual health needs, how they experience pain, and/or which tools are more effective for that individual. The hospital passport should also include any information that the individual may need to access health services.
There are different hospital passports depending on the region or hospital; however, the information within the document should be relatively the same. Staff should request a review of this document to ensure they have a full understanding of the individual before assessment and treatment (where safe to do so). In Wales, it is known as The Once for Wales Health Profile - NHS Wales.
Reasonable adjustments
The Equality Act (2010) states that those with a protected characteristic, including disability, are entitled to reasonable adjustments. The Act highlights that people and organisations have ‘a duty to make reasonable adjustments’ to ensure that people who are disabled are not at a disadvantage.
Organisations have an ‘anticipatory duty’ to make reasonable adjustments before someone needs to ask, for example, building changes/ramps. Reasonable adjustments for those with a disability when accessing health care may include taking additional time to explain information, providing alternative communication aids, such as BSL interpreters or requesting a telephone appointment instead of a face-to-face appointment.
Reasonable adjustments vary for each person and should be considered in anticipation or proactively, where possible. A person’s hospital passport should include references to the reasonable adjustments that would be supportive for someone with a disability.
Further information
Advocacy
An individual with a learning disability may need support from others to advocate their wishes, which is also considered advocacy. They provide support, information and representation to empower individuals with learning disability.
An advocate may be a family member, carer, or an independent advocate within the community. An independent advocate supports ensuring the individual with a learning disability’s voice is heard; this involves spending time with them to understand their wishes, then supporting them to articulate them or create the change they wish for.
It is also important for staff to appreciate what may influence how a carer or close family member communicates with the team caring for their informal caregivers. For instance, they may have had a negative experience in the past or felt unheard, which makes it especially important to take the time during the assessment to ask for their perspective on the current situation. There may also be an underlying fear that their informal caregivers will be denied certain treatment.
Questions for consideration that may be helpful for the carer/professional to ask the family when assessing for pain:
- What makes you think your family member/ patient has pain?
- How do you know when your family member/patient has pain?
- Can you describe any behavioural changes that may indicate pain?
- Have you noticed a change in eating habits, for example, a reduced appetite?
- Have you observed any change in bowel/ urinary habits?
- Is your family member /patient touching or rubbing any part of the body?
- Is your family member/patient more irritable than usual or crying?
Research shows that families and carers often do not receive training on recognising pain responses, despite their key role. Many carers also believe they do not need training, yet misconceptions about health and behaviour can have serious consequences on someone’s wellbeing.
Unidentified pain can lead to repeated acute and psychiatric hospital admissions, often due to familiarity and desensitisation, where health concerns are mistaken for typical behaviour.
Effective communication between health care teams, families, and caregivers is crucial to identifying and addressing pain and distress. Without clear dialogue, vital information may be missed, delaying care and causing unnecessary suffering.
Strong communication is fundamental to person-centred care, particularly for individuals with cognitive impairments or communication challenges, as well as those in palliative or end-of-life care.
Further information
Complexity in communication
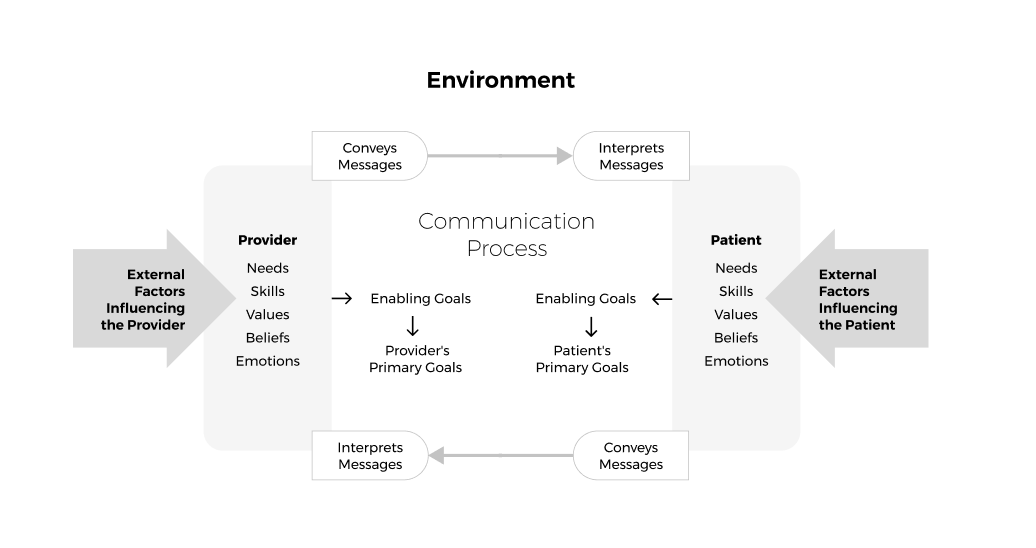
It is important to acknowledge the complexity of communication, as shown in Figure 1 below (developed by Feldman-Stewart in 2005). The model shows how two-way communication between a professional and a patient can be influenced by internal and external factors.
The level of complexity explains how breakdown can occur, as it is usually due to misperceptions of the communication that lead to challenges or misunderstandings.
Figure 3: Conceptual Framework for Patient Professional Communication (Feldman-Steward et al. 2005)
Skills to support effective communication
There are various key skills which are known to support effective communication. These include:
- Active listening (checking out/reflecting).
- Use of open questions.
- Body language (for example, good eye contact).
- The way we respond (for example, being genuine, non-judgemental, honest, with empathy and not using jargon).
These skills can be utilised to apply the principles devised by The World of Work Project in 2019: The 7 C's of Communication. These are a list of principles to guide effective communication as follows:
- Clear.
- Correct.
- Concise.
- Complete.
- Concrete.
- Considered.
- Courteous.
Integral to good communication is self-awareness and considering how we are seen by others when it comes to communicating with patients. Additionally, being self-aware can improve a person’s mental wellbeing from a work perspective.
Paying attention to what their body language is saying is important: does it match their verbal communication? Rather than suggesting what may be sore, use gentle questioning.
Chochinov (2022) describes how body language, including touch, can convey kindness and compassion, thereby supporting the health care professional's perception of the person.
In fact, most of the messages we convey are nonverbal and are about our body language and tone of voice, compared to the actual words spoken. He refers to this as the “care tenor” or “tone of care” and how this has a “profound” influence on a patient's sense of dignity.
Challenges affecting communication
There are many challenges affecting how we communicate, including:
- time
- lack of knowledge
- environment
- remote and rural access
- expectations
- fear
- confidence
- family dynamics
- mode of communication
- cognitive impairment, for example, dementia.
Effective communication between professionals and teams is equally important for achieving the best possible outcomes for patients, but can be complex.
The use of tools can help reduce the risk of misunderstandings or of vital information being missed completely.
Communication tools, such as ‘SBAR’, can also reduce the time required during interactions, enabling a more focused approach to conveying information about a patient to another team or professional at the point of handover or referral.
- S: Situation. A brief description of the situation that has triggered the request for advice/referral.
- B: Background. Provide details of the patient, age, where they live, who they live with, what their normal function is, if they have a disability and/or care package, and what medication is prescribed.
- A: Assessment. Provide a summary of the outcome of assessment, including psychological, spiritual and social, as well as physical needs.
- R: Recommendations. Explain what the request is, for example, what is required of the person contacted (an urgent review or advice?). Explain what your recommendations are.
It is helpful to use a model when having to convey communication that may be difficult for people to hear and receive, for example, the SPIKES Model for Breaking Bad News:
- S: Setting. Try to ensure privacy.
- P: Perception. Establish what the patient/person already knows.
- I: Invitation. Would you like/is it okay for me to share with you?
- K: Knowledge. Share the information after giving a warning, for example, ‘Unfortunately’, or ‘I’m so sorry, but’.
- E: Empathy. Show empathy— give space.
- S: Summary. Summarise the key points of the interaction and the pain.
Phrases to support communication
While having a “script” may cause additional stress for staff, it may be helpful to have some useful phrases to navigate the complexity of some interactions. Some examples include:
- “That sounds really difficult.”
- “I notice… and I wonder…”
- “May I ask what a good day would look like for…?”
- “Would you mind telling me, in your words, what was said at the clinic/by the doctor?”
- “Is it okay if we talk about this?”
- “I am sorry to be having this conversation on the phone. I would rather be with you in person, but obviously, that is not possible today.”
- “I am sorry, I do not know the answer to your questions; it sounds difficult for you. Let me call the nurse/doctor and ask if they can speak with you.”
These phrases can support your communication and gently foster kindness and compassion in all interactions and interventions.
Resource lead
Contact details for the resource lead:
