Pain assessment tools for children and young people
Downloaded content date
Pain assessment tools for children and young people

Several learning disability-specific pain assessment tools can be used for children and young people. The following five tools are highlighted as most beneficial for use with children and young people aged 3 or older.
In deciding which tool to use, it is helpful for carers and clinicians to understand the child or young person’s cognitive ability and communication style.
The tools can be used with younger children, but when caring for a baby, it is recommended to use a specific neonatal pain assessment scale, such as the NIPS (Neonatal Infant Pain Scale).
Please note, we discussed a few of these in the previous section, but this information has been written with a focus on children and young people.
Figure 2. Right tool, right setting, right time, right outcome
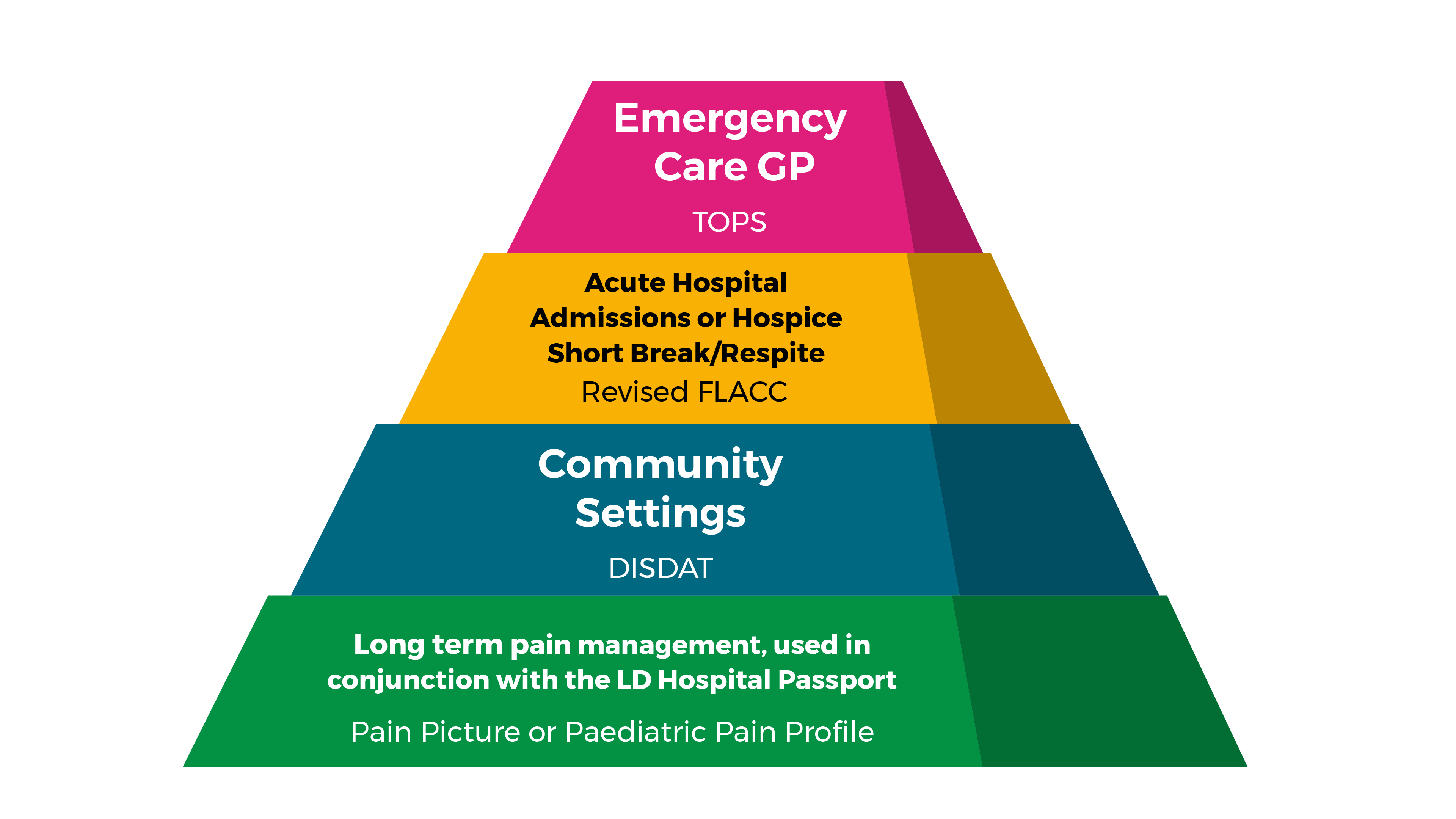
Revised FLACC observation tool
(Acute hospital admissions or hospice short break/respite)
The Revised FLACC scale is appropriate for short-term or inpatient settings where children and young people may be unable to verbally communicate pain. This has a scale of 0-2 for five categories, giving an overall score out of 10.
The categories are face, legs, activity, cry and consoling. It has been well established for young preverbal children. The revised version allows parents to add unique descriptive behaviours for their child/young person.
Advantages
- widely used and recognised within children’s hospitals and hospices internationally
- quick and straightforward to complete
- considers the individual behaviours of each child.
Disadvantages
- some of the descriptions might be the child’s ‘normal’ behaviour, for example, occasional tremors
- might not adequately capture pain behaviours of those with significant limitations in movement.
Paediatric Pain Profile (PPP)
(Long-term pain management)
The Paediatric Pain Profile (PPP) has a 20-item rating scale that assesses behaviour and pain history. Each item is rated on a scale of 0-3 to give an overall score out of 60. The tool went through five stages of development, which are discussed on the PPP website.
Advantages
- descriptive
- includes pain history with pre-identified pain behaviours, causes and management.
Disadvantages
- will require additional time to complete.
DisDAT
(Community settings)
The DisDAT (Disability Distress Assessment Tool) (PDF) is designed for people with severe communication difficulties. It helps carers and clinicians detect distress that may be due to pain or other unmet needs by comparing usual and unusual behaviours.
This is not a scoring tool—it is intended to help identify distress cues by looking at four categories of signs and behaviours. This includes appearance, voice, habits/mannerisms and posture/observations. It is also designed to document a child/young person’s usual content cues, enabling distress cues to be identified more clearly.
Advantages
- personalised
- involves and empowers families
- identifies distress and contentment cues.
Disadvantages
- handwritten only.
TOPS – Tailored Observational Pain Screen (Emergency care/GP)
Use TOPS as a quick and essential screening tool during urgent or emergency presentations. It helps identify immediate physiological changes that may indicate pain or distress. It is an individualised table completed by parents/carers with topics to consider. Space is available for information on pain-relieving strategies, along with an evaluation of these strategies.
Advantages
- personalised, describing specific behaviours for the individual
- may be useful for children with atypical pain behaviours and who lack other typical behaviours that may lead to false low scores on other tools.
Disadvantages
- dependent on how well the behaviours are described
- requires the parent or carer known to the child/young person to be present for assessment.
Pain Picture
(Long-term pain management)
A traffic-light colour scheme is used to highlight the perceived severity of pain. Explicit nursing observations are added to the information provided by the family or carer. The patient’s own experiences are sought where possible.
Advantages
- individualised
- descriptive
- allows for subtle changes to be noted
- suggested intervention options.
Disadvantages
- no template—would need to be created for individual patients
- requires additional time to complete the pain picture.
Behavioural observation tools for children
There may be more scope to use some of the more complex behavioural observation tools that are more involved and require considerable time to populate and use. For example, using the Non-Communicating Children's Pain Checklist (NCCPC) (PDF) or the Paediatric Pain Profile (PPP), when there is complex, uncontrolled pain.
The Revised FLACC scale (PDF) (Face, Legs, Activity, Cry and Consoling), indicates both ‘normal’ and pain-related behaviours, but might not adequately capture pain behaviours of patients with significant limitations in movement.
That is where individualised tools such as the Individualised Numeric Rating Scale (INRS) or Treatment Outcomes in Pain Survey (TOPS) may be useful. These are more patient-specific and can capture subtle, idiosyncratic pain-related behaviours not adequately described by standard tools.
Whatever pain tool is selected, collaboration and input from the parent/carer is essential, to capture their child’s individual pain behaviours.
Resource lead
Contact details for the resource lead:
